
Preventing And Treating Tennis Injuries Of The Lower Extremity

Given the increasing popularity of tennis, more and more players will present with injuries to the heel, Achilles, and ankle. These authors offer expertise on the mechanics of injury as well as exercises you can recommend to players for their rehabilitation to get back on the court.
Tennis has been one of the fastest-growing traditional sports in the United States during the past decade. With an estimated 46 percent increase in the number of participants, tennis has outpaced the growth of other popular sports, including baseball, ice hockey, gymnastics and football.1,2
The sport of tennis has changed significantly in the past 25 years. New equipment, including racquets and polymer strings, has increased the speed of the game even for the recreational player. The physicality of the sport is demanding with rapid changes in direction and frequent stopping and sprinting. Differences in skill level, court surface type, player age and physical conditioning can further influence or complicate injury manifestation.3,4


As a result of these changes, we are seeing an increase in the number of foot, ankle and leg injuries. The treatment and prevention of these injuries continue to change as well. With this in mind, we would like to share our experience with the management of these injuries.
In a prior study on 376 participants, Feit and Berenter determined that common foot and ankle injuries in tennis players included Achilles tendon injuries, plantar fasciitis, ankle sprains, subungual hematomas, muscle cramps and blisters of the feet.5 In recent years, we have seen an increased incidence of hip, hamstring, groin and thigh muscle injuries. We believe the increased speed of the game has contributed to this.


A Closer Look At The Mechanisms Of Tennis Injuries
Understanding the most common strokes in tennis will help the coach and practitioner in the prevention and treatment of these injuries.
When hitting a forehand (see above left photo) or a backhand (see below right photo), most players use an open stance, which places a majority of the stress on the rear hip, thigh and calf during the backswing, and the weight transfers to the opposite foot after contact with the ball. The player is more prone to a muscle injury of the hip, thigh or groin. After one hits a wide forehand or backhand shot, the groin and ankle are prone to injury as the player tries to plant the outside foot and recover back into the court.
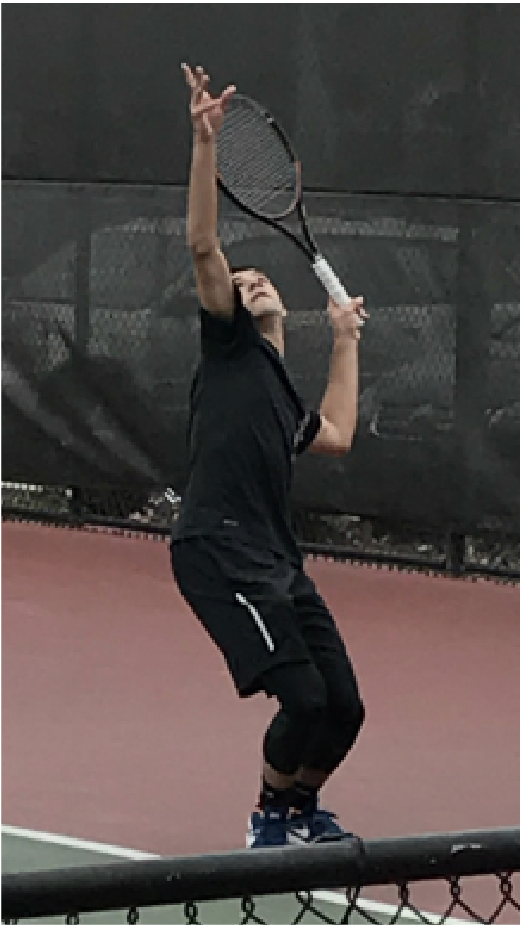
When hitting a serve, the calf muscle and Achilles tendon are most prone to injury, which is a result of stress on the legs and hips during the ball toss. Then there is a rapid jump to make contact with the ball and a forceful landing on the the back leg during the follow through as the back leg moves forward into the court (see photos below). The gastrocnemius muscle is susceptible to injury when a rapid eccentric contraction occurs as the foot experiences rapid dorsiflexion in the presence of knee extension. Although this is common when serving, it may also occur after an overhead smash or when chasing after a short ball.5
When Tennis Players Develop Muscle Strains
The most common muscle strains in tennis players are to muscles like groin and calf muscles that cross two joints. Injury most often occurs when the efforts of the adductors and hip flexors are opposed by lateral momentum, and contraction results in muscle tearing rather than the anticipated deceleration.6
Predisposing factors to muscle strains include muscle weakness, muscle imbalance and a lack of flexibility of muscles and the associated ligaments.7,8 The hamstrings, another common site for injury, should be at least 60 percent as strong as the quadriceps or injury to these muscles is likely.9,10 In recent years, players have been hitting forehand shots with the majority of the weight on the leg farthest from the net in an open stance position (see above left photo) As a result, players often develop one leg that is stronger than the other, which potentiates injury.
Many young tennis players often have weak lower extremity muscles and therefore do not have sufficient strength to hit the ball the way older players do. They must instead rely on biomechanical efficiency and looser string tension to hit the ball with more pace. If there are deficits anywhere in the kinetic chain, there will be an increased load of other joints and muscles, which leads to increased injury risk.8
Patients with hamstring and groin injuries commonly receive physical therapy including phonophoresis, electrical stimulation, taping and ice. These injuries will often keep a player off the court for two to six weeks, depending on the severity of the strain or tear. Continuing to play on the injury will only make it worse.
The calf muscle is a very common site of injury. The medial head of the gastrocnemius muscle is the site of predilection for calf muscle tears.11,12 The mechanism of injury is the result of a sudden step or jump producing an acutely painful situation that players describe as having been struck hard with a club on the back of the calf.
When it comes to calf muscle strains, patients typically receive physical therapy modalities including phonophoresis, electric stimulation and passive motion exercises. Immobilization is not recommended unless it is a severe tear or there is Achilles tendon involvement. Patients should apply topical anti-inflammatory gel in the form of diclofenac gel three times a day and seek treatment with a physical therapist.
Keys To Addressing And Preventing Achilles Tendonitis
Achilles tendon injuries may be acute or chronic. A sudden significant increase in activity or the effect of long-term repetitive stress on the tendon may lead to the development of microtears with or without calcium deposits, or degenerative changes. The area located 2 to 6 cm above the insertion of the Achilles tendon in the posterior aspect of the heel is the most common site of injury. This region of the tendon has poor vascularity and is more prone to injury. Calcaneal eversion, a plantarflexed first ray, flexible forefoot valgus and abnormal pronation may contribute to this injury as well.13,14Rapid, abnormal pronation in gait results in a whipping action of the Achilles tendon, producing an increase in friction between the tendon and peritenon.
Initial treatment for Achilles tendonitis should include a heel lift, ice, topical diclofenac gel, a night splint and rest. If the patient is limping, controlled ankle motion (CAM) walker immobilization may be needed for two to four weeks prior to physical therapy and rehab exercises.
Once the inflammation resolves, we recommend custom orthotics that would include a semi-rigid material (i.e., polypropylene). This material will have some flex when the patient is playing but still provide adequate support. We do not recommend rigid materials for tennis players. A rearfoot post is needed with Achilles tendon injuries to help prevent overstretching of the tendon and further injury. Top covers with nylene and Poron will provide more shock absorption and minimize stress on the lower extremity.
Pertinent Insights On Ankle Sprains
An ankle sprain is a common injury that will prevent the player from competing for two to six weeks, depending on the severity of the sprain. The most common mechanism involved is a plantar flexion inversion type injury. Etiologic factors that predispose the athlete to ankle sprains include a rigid forefoot valgus or plantarflexed first ray, rigid or high degrees of rearfoot varus, limited ankle joint dorsiflexion, intoeing conditions, limb length discrepancy, muscle imbalance or weakness, fatigue, ligamentous laxity, shoes and playing surface.15
Treat grade 1 ankle sprains with ice, compression and proprioceptive exercises. Grade 2 ankle sprains require CAM walker immobilization for two to four weeks followed by the use of an ankle brace. Physical therapy is very helpful after three weeks to help reduce the pain and inflammation. A popular ankle brace for college and professional players is the ASO ankle brace, which patients wear over a sock and has laces with Velcro straps for support. Taping is not as popular anymore as we have found it often loosens up 50 percent after one hour of use. Patients can tighten ankle braces periodically as needed if they are wearing them while playing.
Grade 3 ankle sprains will require more time off the court as they often require six weeks of immobilization in a CAM walker and ankle brace, and then at least four weeks of physical therapy prior to the patient returning to the court. Even after the ankle heals from a sprain, we recommend using an ASO ankle brace for at least one year after the injury for grade 2 or grade 3 sprains to help prevent recurrence. Despite proprioceptive exercises, the ankle is vulnerable to recurrence with the physical demands of playing tennis.
How Can Tennis Players Recover From Plantar Fasciitis?
Pain in the heel and arch is a common injury in tennis players. This injury is a result of chronic overuse caused by microtearing of the fascia fibers secondary to longitudinal midtarsal joint supination with subtalar joint pronation. The microtearing that occurs initiates an inflammatory response in an attempt to repair the damaged fibers. The pain produced is most often localized to the attachment site of the plantar fascia at the medial tubercle of the os calcis. Pain may be most severe when taking the first few steps out of bed in the morning or when warming up to play tennis. The pain may gradually lessen with exercise only to return after a period of rest.
Treatment for plantar fasciitis should initially include ice, calf stretching, over-the-counter orthotics, oral anti-inflammatories and using more supportive shoes. If the pain persists, treatment often includes a night splint and a corticosteroid injection. For long-term pain relief and prevention of recurrence, we often recommend custom orthotics. We recommend a semi-rigid polypropylene device with a soft top cover. Research has shown that custom orthotics help reduce peak pressures on the feet at specific plantar regions, which will help prevent recurrence of the injury.16
Preventing Injuries Before Athletes Take The Court
Fitness training has evolved in recent years to help prevent injuries and enhance play. Prior to playing, patients often perform dynamic exercises to help warm up the hamstring, groin and hip muscles. This may include straight leg swings, skipping, light jogging and side to side shuffling. After playing, static stretching and yoga exercises are the most important factors in muscle recovery and maintaining elasticity of the muscles. Professional players such as Roger Federer and Novak Djokovic will often spend 30 to 60 minutes stretching and doing yoga-type exercises after a match or long practice.

The top five most important stretches or yoga positions after practice include hamstring stretching with a strap or elastic band. The safest way to do this stretch is while the patient is lying on his or her back, and keeping both legs straight. Then the patient should slowly elevate one leg with the use of the strap until he or she feels resistance. Have the patient hold the stretch for at least 30 seconds. It is vital to also stretch the iliotibial band at the same time. The iliotibial band often contributes to knee and thigh injuries. The patient can also stretch the iliotibial band easily while lying on his or her back by simply moving the leg medially with the strap.
Other vital stretches include the crescent lunge, which will stretch the plantar heel and arch, hip, calf and thigh muscles. The groin and quadriceps stretches are also essential after playing.
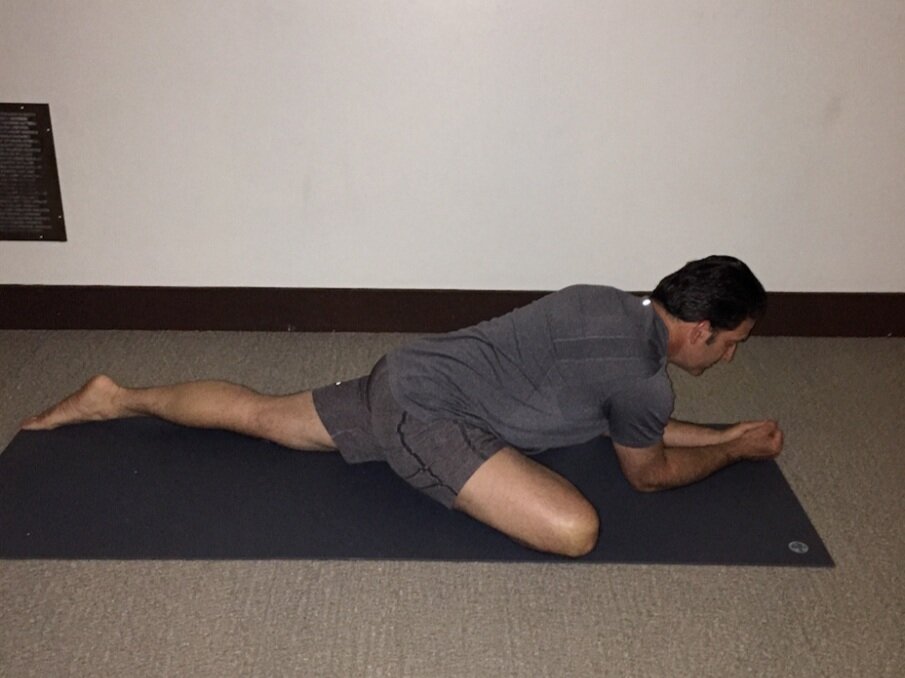
Another important yoga stretch after playing is the pigeon pose, which creates a deep hip opening while also stretching the quadriceps and hip flexors for the side of the upper leg (see left photo).
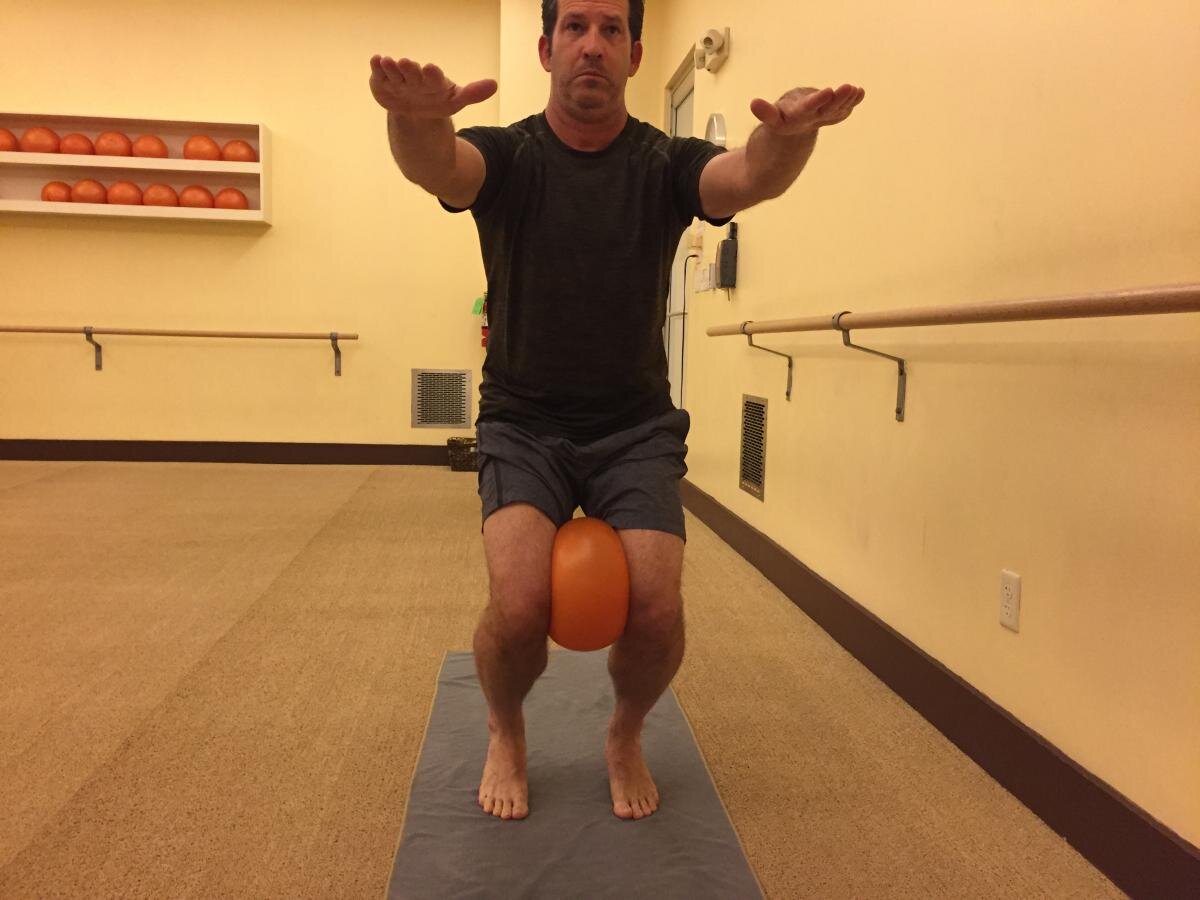
Strength training is a vital part of a tennis player’s training not only to help improve his or her game but help prevent injury as well. Some exercises that are very helpful are lunges, rotational exercises with a medicine ball and balance exercises with the feet flat or the heels raised in a semi-seated position known as a chair pose (see below photos). When performing this exercise with a medicine ball, patients will strengthen core muscles as well as the peroneals, calf and quadriceps.
What You Should Know About Knee Injuries On The Tennis Court
The sharp side-to-side movements in tennis predispose the athlete to significant valgus and rotary stresses on the knee. The most common injuries include patellar tendonitis, patellofemoral pain, meniscus injuries and cruciate ligament damage. These side-to-side movements require pushing off with the knee in a flexed, valgus and externally rotated position. This places abnormal lateral forces on the knee extensor mechanism, contributing to injury. Some predisposing factors to knee injuries in tennis players include playing surface, shoe gear, increased femoral anteversion, increased external tibial torsion, increased genu valgum and excessive foot pronation.17,18
Patellar tendonitis is a common knee injury in tennis. This may be caused by the constant bending, jumping and pushing off during the recovery of wide shots. This repetitive action leads to fatigue and tissue microtearing at predisposed areas near the insertion of the patellar tendon. Microtearing often occurs at the lower pole of the patella. A hypermobile patella or tight iliotibial band are often etiologic factors in patellar tendonitis.19,20 Treatment often includes ice, physical therapy and use of a patellar tendon strap/brace.
Dr. Feit is in private practice in Torrance and San Pedro, Calif. He is the President of Precision Foot and Ankle Centers.
Dr. Kashanian is in private practice in Torrance and San Pedro, Calif.
Mr. Feit is a research assistant at Precision Foot and Ankle Centers.
References
United States Tennis Association. Tennis fastest growing sport in America. Available at www.usta.com .
Gaw C, Smith G. Tennis related injuries treated in United States emergency departments, 1990-2011. Clin J Sport Med. 2014; 24(3):226-232.
Perkins RH, Davis D. Musculoskeletal injuries in tennis. Phys Med Rehabil Clin N Am. 2006; 17(3):609-631.
Bylak J, Hutchinson MR. Common sports injuries in young tennis players. Sports Med. 1998; 26(2):119-132.
Feit EM, Berenter R. Lower extremity tennis injuries: prevalence, etiology, and mechanism. J Am Pod Med Assoc. 1993; 83(9):509-514.
Balduini FC. Abdominal and groin injuries in tennis. Clin Sports Med. 1988; 7(2):349–57.
Liemohn W. Factors related to hamstring strains. J Sports Med. 1978; 18(1):71–6.
Hjelm N, Werner S, Renstrom P. Injury risk factors in junior tennis players: a prospective 2-year study. Scand J Med Sci Sports. 2012; 22(1):40-48.
Burkett LN. Causative factors in hamstring strains. Med Sci Sports. 1970; 2(1):39–42.
Casperson PC. Groin and hamstring injuries. Athlete Train. 1982; 17(1):43.
Miller WA. Rupture of the musculotendinous juncture of the medial head of the gastrocnemius muscle. Am J Sports Med. 1977; 5(5):191–3.
Millar AP. Strains of the posterior calf musculature. Am J Sports Med. 1979; 7(3):172–4.
Leach RE. Achilles tendinitis. Am J Sports Med. 1981; 9(2):93–8.
Nelen G. Martens M. Surgical treatment of chronic Achilles tendonitis. Am J Sports Med. 1989; 17(6):754–6.
Petrov O, Blocher K. Footwear and ankle stability in the basketball player. Clin Pod Med Surg. 1988; 5(2):275–90.
Hodge MC, Bach TM. Orthotic management of plantar pressures and pain in rheumatoid arthritis. Clin Biomech. 1999; 14(8):567-575.
Gecha SR, Torg E. Knee injuries in tennis. Clin Sports Med. 1988; 7(2):435–52.
Milgrom C, Finestone A. Patellofemoral pain caused by overactivity: a prospective study of risk factors in infantry recruits. J Bone Joint Surg. 1991; 73A(7):1041–3.
Ferretti A, Ippolito E. Jumper’s knee. Am J Sports Med. 1983; 11(2):58–62.
Martens M. Wouters P. Patellar tendonitis: pathology and results of treatment. Acta Orthop Scand. 1982; 53(3):445–50.
For further reading, see “Key Insights On Treating Tennis Injuries” in the August 2005 issue of Podiatry Today or “Pertinent Insights On Preventing Injuries On Tennis Court Surfaces” at http://tinyurl.com/go7kd34 .